Direct Access Colonoscopy (DAC) Services in NSW
What is a colonoscopy?
Following a positive bowel screening result, a General Practitioner (GP) will refer a patient to have a colonoscopy for further investigation. During the procedure, a doctor will insert a narrow flexible tube with a tiny camera into the bowel to look for polyps or cancerous growths.
For more information, visit this helpful website.
Ways to access a colonoscopy in NSW
There are three main pathways a patient can take to access a colonoscopy in NSW. The pathway they take will affect:
- how they are assessed prior to the procedure (in person or over the phone)
- the out-of-pocket costs associated with the pre-colonoscopy assessment
- the colonoscopy itself
- the time they will need to wait to have their colonoscopy.
It’s important for patients to be fully informed of the options available to them. They should also be informed of financial or other implications prior to being referred.
Following a positive bowel screening result, a GP will refer a patient to:
- 1. The Direct Access Colonoscopy (DAC) service of a public hospital
Most patients will be assessed over the phone prior to the day of the colonoscopy. There will be no out-of-pocket costs to the patient for either the pre-colonoscopy consultation or the procedure itself. More details below. - 2. The outpatient gastroenterology clinic of a public hospital
The patient will need to attend the hospital in person to be assessed prior to the day of the colonoscopy. There will be no out-of-pocket costs to the patient for the pre-colonoscopy consultation or the procedure itself if the colonoscopy is then done in a public hospital. - 3. A private specialist’s (gastroenterologist or colorectal surgeon) rooms
The patient will typically need to be seen in person to be assessed prior to the colonoscopy which often incurs an out-of-pocket cost.
This page focuses on option 1 (Direct Access Colonoscopy).
What is Direct Access Colonoscopy (DAC) and what are the benefits?
DAC is a NSW Health Leading Better Value Care initiative that focuses on helping people gain access to public colonoscopy services after a bowel cancer screening test. This test is known as an immunochemical Faecal Occult Blood Test or iFOBT.
A key advantage of DAC is that it allows otherwise healthy patients, who have a positive iFOBTto be assessed and triaged during a free telephone appointment with a trained nurse. This is an alternative to having a face-to-face appointment with a specialist prior to the day of the colonoscopy.
The benefits of this service is that it:
- removes the wait for a public outpatient consultation, for suitable patients
- allows direct booking to colonoscopy
- frees up clinic time for patients with more complex issues.
If patients are suitable for telephone assessment, they will only need to come in person once for their actual procedure.
DAC services improve access to colonoscopy for people in NSW by reducing barriers commonly faced by patients, such as:
- extended wait times for clinic appointments
- unnecessary face to face appointments
- the need to take time off work
- time spent travelling to specialists/outpatient appointments
- out-of-pocket costs for private specialist room appointments.
What if the patient doesn’t meet the referral criteria for the triage in a DAC service, or if they aren’t able to be triaged by telephone?
They will need to make a face-to-face appointment in clinic with a specialist before their colonoscopy.
Direct access pathway for positive iFOBT

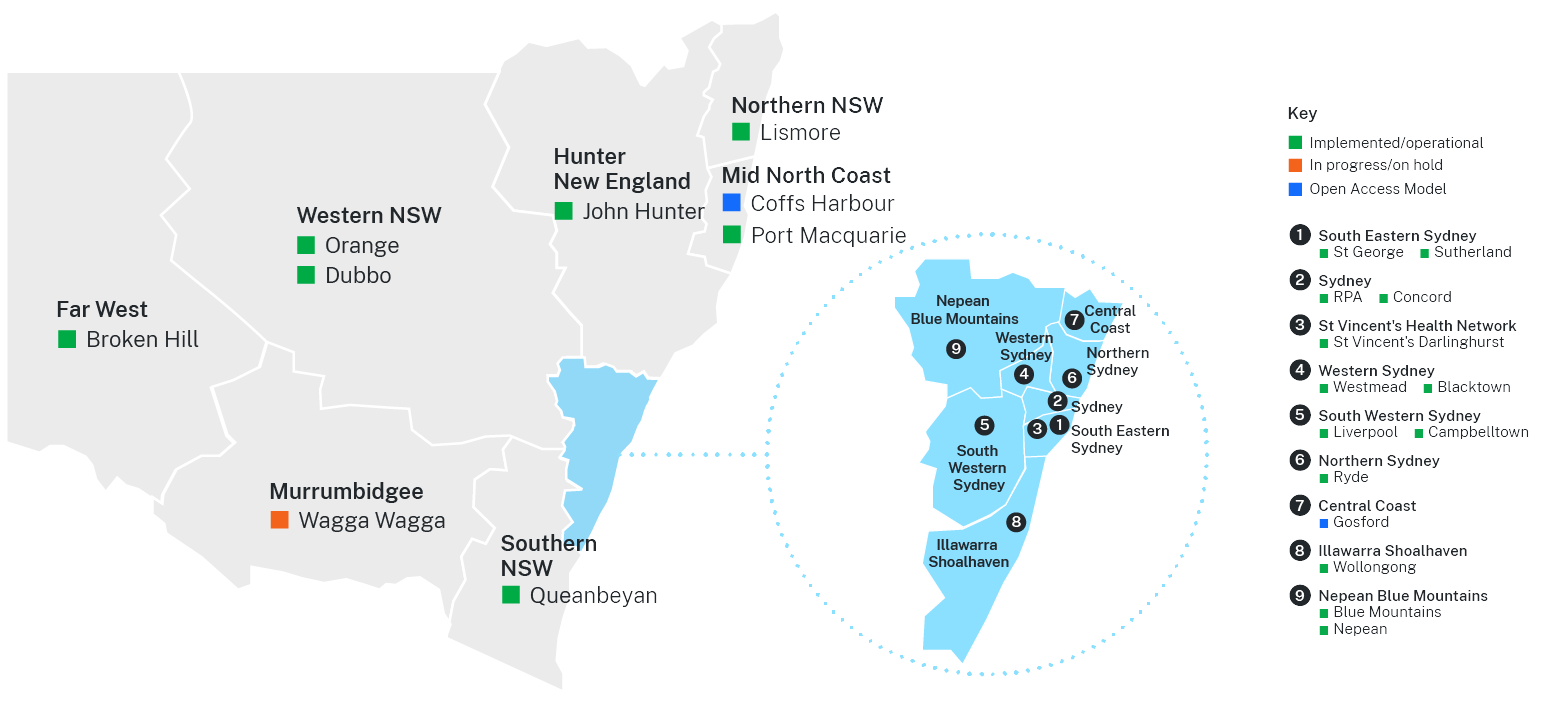
Where are the DAC services in NSW?
There are 21 established DAC services across NSW. Most Local Health Districts (LHDs) have at least one operational DAC service available. Please see the map below to find your nearest available DAC service.
Information for primary care providers
Why should I refer my patients to DAC?
A DAC service aims to mitigate the impact of the common barriers faced by patients by allowing clinically eligible patients to be assessed over the telephone by a Clinical Nurse Consultant. A nurse-led telephone triage assessment enables patients meeting the inclusion criteria (see below) to be referred directly to a DAC service, whilst also allowing specialist clinic time to be directed to more complex patients. DAC services have a well-structured and protocolised triage and assessment pathway which assures safe, independent assessment by nursing staff with specialist oversight.
DAC is a beneficial option for clinically eligible patients leading to:
- The earlier detection of bowel cancer which should lead to a lower incidence of bowel cancer and reduced morbidity and mortality for patients.
- Improved access to public colonoscopy, especially in areas without an existing outpatient clinic.
- Improved wait times for colonoscopy resulting from the removal of the wait for a face-to-face pre-colonoscopy clinic appointment.
- Reduced anxiety and psychological distress (resultant from lengthy waiting periods).
- For public hospitals and specialists, a reduction in low-value clinic activity (redirecting patients who do not need to be seen in person to DAC assessment) and therefore increasing the service’s capacity to focus on more complex cases.
- Reduced out of pocket costs and travel time for patients.
Who is eligible to be referred to a DAC service and how do I refer to DAC?
Each DAC service has developed their own clinical criteria specific to their local circumstances and population, however, in general the referral criteria requires a patient aged 50-75 years to have returned a positive iFOBT, be asymptomatic and be otherwise healthy.
Refer to the table below to be directed to your local HealthPathways colonoscopy information page for region-specific eligibility criteria and referral information.
If you do not use HealthPathways, please refer to the ‘alternative referral contact details’ column below.
Region |
HealthPathways:
|
HealthPathways:
|
Alternative referral contact details |
|
ACT Health/Southern NSW |
Queanbeyan DAC Clinic: |
||
|
Sydney |
RPAH DAC Clinic: Concord Hospital DAC Clinic: |
||
|
St Vincents Hospital Network |
St Vincents Hospital DAC Clinic: |
||
|
South Eastern Sydney |
St George Hospital DAC Clinic: Sutherland Hospital DAC Clinic: |
||
|
Hunter New England |
John Hunter Hospital (SeNT eReferral form) |
John Hunter Hospital DAC Clinic: |
|
|
Central Coast |
Central Coast Gastroenterology Gosford: |
||
|
Murrumbidgee |
Wagga Wagga Base Hospital** |
In progress |
To be confirmed |
|
Nepean Blue Mountains |
Blue Mountains DAC Clinic: Nepean DAC Clinic: |
||
|
North Coast |
Lismore Base Hospital** |
|
To be confirmed |
|
Mid North Coast |
Port Macquarie Base Hospital: Coffs Harbour Health Campus: |
||
|
Illawarra Shoalhaven |
Wollongong Hospital Gastroenterology: |
||
|
Sydney North |
Ryde Hospital DAC Clinic: |
||
|
South Western Sydney |
Liverpool and Campbelltown FOBT DAC Clinics: |
||
|
Western NSW |
Broken Hill Hospital Dubbo Health Service Orange Health Service |
|
Orange Health Service DAC Clinic: Dubbo Health Service DAC Clinic: Broken Hill Base Hospital DAC Clinic: |
|
Western Sydney |
Westmead Rapid Access FOBT Clinic: Blacktown Rapid Access FOBT Clinic: |
* Open Access Colonoscopy (OAC) Model: An OAC is an alternate referral pathway allowing a GP to refer directly to an endoscopist without a specialist appointment prior to colonoscopy. This model differs from a DAC model due to the absence of nurse-led assessment and triage as well as a lack of overarching specialist oversight.
** These services will start taking referrals in 2024. Referral links to be updated when available.

DAC model of care
The DAC model of care (PDF) provides guidance for the localised implementation of direct access services across NSW. The model of care outlines the mandatory and recommended inclusions for implementation and should be read in conjunction with the following:
- the Australian Commission on Safety and Quality in Health Care Colonoscopy Clinical Care Standard 2018
- the National Safety and Quality Health Service Standards
- the National Health and Medical Research Council (NHMRC) Clinical Practice Guidelines for Surveillance Colonoscopy
- local LHD and SHN policies and procedures.
In 2024, the model of care was revised to ensure accuracy and to incorporate any changes to practice since the model was first published in 2020.
